Alternative Insight
Health is a Socio-Economic Problem
Note: This is an update of an earlier and timely article.The recent debates on health plans have omitted a vital aspect of the discussion - recent reports have shown that a large inequality in the distributions of wealth and income are more significant factors than either absolute poverty or low income in determining the health of deprived populations. Despite these published reports, the United States government and the medical profession neglect the data and refuse to propose programs that will modify the socio-economic system in a manner that improves the health of all of its citizens. The neglect creates a serious problem; citizens' security and health are threatened and therefore the security and health of the nation are also threatened.
Let's start with brief descriptions of research that support the theses that social status and distribution of income determine the quality of health.
The Research
CAUSE OF DEATH: INEQUALITY. Dollar & Sense, May, 2001, Alejandro Reuss
Men with less than 12 years of education are more than twice as likely to die of chronic diseases (e.g., heart disease), more than three times as likely to die as a result of injury, and nearly twice as likely to die of communicable diseases, compared to those with 13 or more years of education. Women with family incomes below $10,000 are more than three times as likely to die of heart disease and nearly three times as likely to die of diabetes, compared to those with family incomes above $25,000. African Americans are more likely than whites to die of heart disease; stroke; lung, colon, prostate, and breast cancer, as well as all cancers combined; liver disease; diabetes; AIDS; accidental injury; and homicide. In all, the lower you are in a social hierarchy, the worse your health and the shorter your life are likely to be.Numerous studies suggest that more unequal income distribution in a country, state, or city lowers the life expectancies for persons at all income levels. One study published in the American Journal of Public Health, for example, shows that U.S. metropolitan areas with low per capita incomes and low levels of income inequality have lower mortality rates than areas with high median incomes and high levels of income inequality. Meanwhile, for a given per capita income mortality rates always decline as inequality declines.
Kawachi, I. and B.P. Kennedy, 1997, Socioeconomic Determinants of Health: Health and Social Cohesion: Why Care About Income Inequality?, British Medical Journal, 314: 1037-1040
Growing evidence suggests that the distribution of income–in addition to the absolute standard of living enjoyed by the poor–is a key determinant of population health. A large gap between rich people and poor people leads to higher mortality through the breakdown of social cohesion. The recent surge in income inequality in many countries has been accompanied by a marked increase in the residential concentration of poverty and affluence. Residential segregation diminishes the opportunities for social cohesion. Income inequality has spillover effects on society at large, including increased rates of crime and violence, impeded productivity and economic growth, and the impaired functioning of representative democracy. The extent of inequality in society is often a consequence of explicit policies and public choice. Reducing income inequality offers the prospect of greater social cohesiveness and better population health.In wartime Britain, narrowing of income differentials was accompanied by a greater sense of solidarity and social cohesion as well as dramatic improvements in life expectancy. In contrast, in the originally closeknit town of Roseto, rapid economic change in the 1960s opened the gap between rich people and poor people. The resulting breakdown of community cohesion was followed by a sharp increase in deaths from coronary disease
Health disparities and the law: wrongs in search of a right.
American Journal of Law & Medicine, Summer-Fall, 2003, Mary A. Bobinskiln
The perhaps unexpected influence of socioeconomic factors can be seen when comparing the data on life expectancy in the United States with that found in other countries. The life expectancy for women in the United States is lower than it is in eighteen other countries; in life expectancy for men, the United States ranks twenty-fifth.Socioeconomic status, as measured either by income or level of education, is strongly correlated with health status.
Healthy People 2010:
In general, population groups that suffer the worst health status also are those that have the highest poverty rates and the least education. Disparities in income and education levels are associated with differences in the occurrence of illness and death, including heart disease, diabetes, obesity, elevated blood level, and low birth weight. Higher incomes permit increased access to medical care, enable people to afford better housing and live in safer neighborhoods, and increase the opportunity to engage in health-promoting behaviors.A note on the effect of unemployment on mortality. Gerdtham UG, Johannesson M., Department of Community Medicine, Malmo University Hospital, Lund University, Malmo, Sweden. ulf.gerdtham@smi.mas.lu.se
Unemployment significantly increases the risk of being dead at the end of follow-up by nearly 50% (from 5.36 to 7.83%). In an analysis of cause-specific mortality, we find that unemployment significantly increases the risk of suicides and the risk of dying from "other diseases" (all diseases except cancer and cardiovascular), but has no significant effect on cancer mortality, cardiovascular mortality or deaths due to "other external causes" (motor vehicle accidents, accidents and homicides).University of Chicago, Nov, 16-22, Sir Michael Marmot, The Social Determinants of Health and Disease Health
One of the dominant features affecting the health situation of all industrialized countries is the social gradient in health and disease. Analysts who approach this topic commonly think of it as a problem of poor health for the disadvantaged and good health for those who are not in the disadvantaged category. This is an inadequate way to pose the problem. The Whitehall Study of civil servants showed that, amongst people who are not poor, there is a social gradient in mortality that runs from the bottom to the top in each society. People in each socio-economic category have worse health than those above them in the hierarchy. Data from the United States confirmed this pattern. In seeking to understand causes for the social gradient it is worth making two observations. First, it applies in non-human primates and other social animals: the lower the status the higher the disease risk and the shorter the life-span. Second, it applies to many societies and different time periods.The research and analysis that demonstrate the significance of effect of disparity in income on health emphasizes the unwillingness of social, medical and economic disciplines to validate the research. During the last century, advances in health were more due to advances in the socio-economic system, and much less to medical advances.
The 20th Century Advances in Health
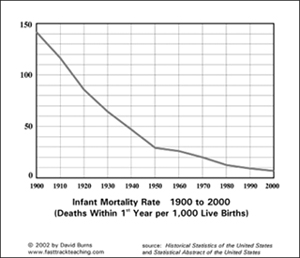
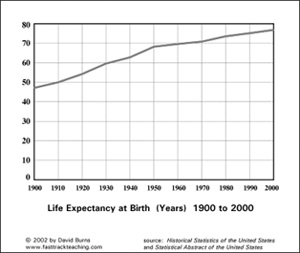
The medical profession credits the decrease in mortality and the conquering of many communicable diseases to the discoveries and uses of vaccines and antibiotics. Historical trends on mortality and disease clearly indicate that the infant and adult mortality rate steadily declined due to the economic benefits of the industrial revolution, which included improved scientific knowledge, increased incomes, improved health care and nutrition. At the same time government regulation and social factors enabled cleaner water and safer environments. Although the introduction of vaccines and antibiotics have had a role in controlling communicable diseases, these diseases were already on a decline before modern controlled methods.Conclusion: Social and economic factors have been large determinants in the increase in longevity and the decline of communicable diseases. Attention to these same socio-economic factors can advance individual health in the 21st century similar to the advances made the 20th century. Some statistics:
Historical data indicates that social and economic progress, and not medical intervention, has been the more significant factor in advancement of American public health. Why aren't government and private institutions giving more attention to the benefits of the social factors? Research by competent and well-recognized investigators highlight the effects of the socio-economic system on the health of the populace. Why aren't these investigations being widely distributed, and why aren't they being used to clarify directions to improve public health? The reason: Pure neglect.
The Neglect
The U.S. government defines the security and health of the American nation as the security and health of the economic system and its industries. It is taken for granted that if the economic system is growing then the citizens will be healthier. This narrow thinking works against the lower economic classes of society. Some thoughts:
- Those who control the economic and political reins of society don't experience the inequalities in the system and don't suffer economically, socially and psychologically from the discrepancies. The system leaders have no direct interest in changing the system.
- Those who suffer from the inequalities don't have the power, the finances, the organization and the political muscle to make their case heard.
- The system is guided by investment leading to profit, rather than investment leading to public health. Investment demands proof that reducing inequalities will provide profits.
- A propaganda machine publicizes economic inequality as beneficial for investment and growth.
- The drug and medical industries benefit financially from the supposition that they provide the unique solutions to health problems. Large research grants enable them to develop products. Afterwards, they convince the public that the investment in the developments must be recouped from the pricing of products. The drug and medical institutions discourage solutions other than their own for resolving health problems.
- The health inequality is treated as a system cost that is less than the financial burden to cure it.
- Government and industrial leaders are ignorant of the data that describes the effects of social and economic inequality upon the public health.
What can be done to improve the health of a populace?
The principal method to improve the health of a population is to respond to the neglect that causes ill-health.
- If social and economic inequalities cause inequalities in health, then it's obvious that reducing the former will reduce the latter. This means attacking the wage and benefit scales from both sides; increasing wages and benefits for the less fortunate and reducing the wages and benefits for the more fortunate. Why should the person who labors at irregular hours to clean a floor be much less rewarded than the person who walks the floor and labors easily during regular hours? Income can be more fairly distributed with total wages and benefits in the system remaining the same. The health will increase for those presently at the low end of the scale and will stay the same for those at the high end of the scale.
- Those who claim that substantial income differentials are necessary for a growing society should be forced to prove their argument. Many nations, especially those in the European Union, which have less economic inequalities, have powerful economies, even with less resources then the nations that have large inequalities.
- The United States government has successfully regulated behavior (tobacco laws, intravenous users, and pollution), and this type of regulation has greatly improved the health of its citizens. The government has also regulated the economic system (minimum wage laws, anti-trust laws, communication and exchange commissions, and banking laws) and this regulation has served to improve the health of its citizens. The government can do more for public health by applying pressure that narrows income distribution.
- Historical trends in improved health, reduced infant mortality, and reduction in communicable diseases clearly show that the social factors of education and sanitation, environmental factors of cleaner water and air and the economic factor of increased prosperity for all have been major in these improvements. It seems conclusive that attention to social and economic factors can be significant in improving public health. More research into the effects of these factors upon health can be instrumental in improving health.
- The drug and medical industry have overrated their performances. Statistics show that drugs have not been the major reason for the decline in many diseases. The medical industry has not greatly reduced pneumonia, cancer, diabetes and the annual return of influenza. Disease resistance to drugs have been noticed. As one example, gonorrhea has been declared resistant to known drugs. An examination of the drug culture and its benefits should be made.
- Although treated with skepticism, the Health Maintenance Organizations (HMO), who want to lower costs, are eager to improve the health of all citizens. HMOs have a part to play in the health debate.
- If it is true that the social and economic inequalities are more significant than the absolute social and economic level, then programs that realign populations, such as low income housing in high income areas, might be counterproductive.
Indeed, not all studies have shown that poor people have worse health if they live in a poor area rather than in a rich one. This lack of unanimity may be the result of the sense of relative deprivation running counter to the effects of the wider environment: a poor person living in an affluent area may have a better environment but may also feel relatively poorer.(Kawachi, I. and B.P. Kennedy, 1997, Socioeconomic Determinants of Health: Health and Social Cohesion: Why Care About Income Inequality?, British Medical Journal, 314: 1037-1040)
Deprived groups don't want to be parted from their environment. Living in the same impoverished manner, but close to groups that emphasize the inequality might be more punishing than living with others at the same low economic leve. Improving the impoverished environment is more rewarding than shuffling people to other neighborhoods so they can observe how they should live. Many programs for alleviating the burdens of the less fortunate have proved ineffective and have only served as token gestures to pacify those desiring system improvements. Only direct attacks on social and economic inequalities can be effective.
The jury is in: The social-economic system that has great inequalities and doesn't properly reward all of its people is detrimental to the health of a major part of its population. The mechanism for resolving the problem is obvious - narrow the distribution of wealth in the system.
alternativeinsight
March 1, 2006
updated oct. 1, 2009
HOME PAGE MAIN PAGE 
alternativeinsight@earthlink.net comments powered by Disqus